Disability Certificate Format In Word for Free Download
Sample Disability Certificate Format is available for free download in MS Word and MS Excel. This sample disability certificate template is normally used to get government benefits for disabled children or persons and get jobs in the government sector or in multinational companies.
Certificate of disability includes the type of disability and cause of disability as evidence with recommendations to perform jobs or any special tasks where the disability doesn’t matter or disturb the performance of a disabled person.
This certificate can be issued by govt departments on a simple letterhead or in printed certificate format. Doctors and Hospitals can also use this format to issue disability certificates or recommend the person get a disability certificate with this template.
Please check the text body of a disability certificate taken from a government document. Please copy and paste in Word, excel, canva, or online editors like live documents or Google document platforms and design according to your needs. Republishing this certificate is prohibited for more information, please check our terms of use.
Disability Certificate
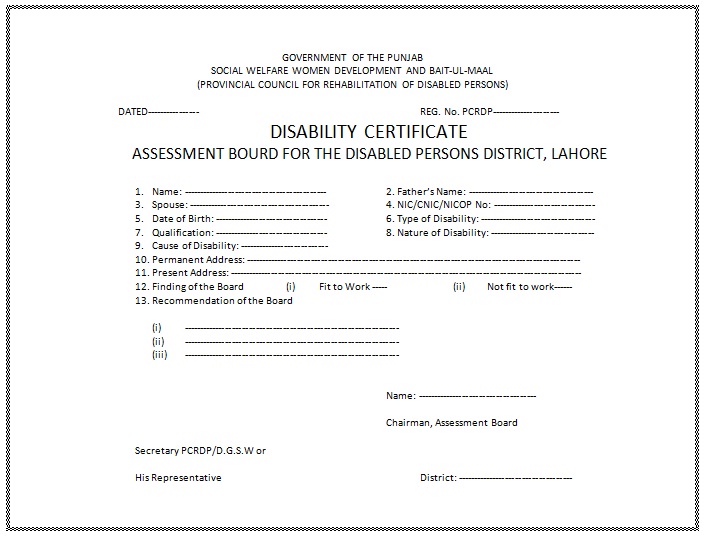
GOVERNMENT OF THE __________
SOCIAL WELFARE WOMEN DEVELOPMENT AND BAIT-UL-MAAL
(PROVINCIAL COUNCIL FOR REHABILITATION OF DISABLED PERSONS)
DATED:—————- REG. No. PCRDP:—————-
DISABILITY CERTIFICATE
ASSESSMENT BOARD FOR THE DISABLED PERSONS DISTRICT, LAHORE
- Name: ————— 2. Father’s Name: ——————
- Spouse: ———– 4. NIC/CNIC/NICOP No: —————
- Date of Birth: ————- 6. Type of Disability: ————–
- Qualification: ————– 8. Nature of Disability: ——————
- Cause of Disability: —————
- Permanent Address: —————————————————
- Present Address: ——————————————————
- Finding of the Board
(i) Fit to Work —– (ii) Not fit to work —— - Recommendation of the Board
(i) —————————————-
(ii) —————————————-
(iii) —————————————
Name: ————————————
Chairman, Assessment Board
Secretary PCRDP/D.G.S.W or
His Representative District: ————-
Format 2: Medical Professional-Issued Disability Certificate
[Official Logo/Heading of Issuing Medical Facility or Clinic] [Address of the Medical Facility] [City, State, ZIP Code] [Phone Number] [Email Address (if applicable)] [Website (if applicable)]
DISABILITY CERTIFICATE
[Issuing Authority’s Seal/Stamp]
This is to certify that Mr./Ms. [Full Name of the Person] with the following details:
- Date of Birth: [Date of Birth]
- Gender: [Male/Female/Other]
- Address: [Full Address]
Has been examined and diagnosed by [Doctor’s Full Name], [Doctor’s Medical License Number], at [Medical Facility/Clinic Name], and has been found to have a disability as defined by [Applicable Law/Regulation]. The disability is of a nature that significantly impairs their daily life activities and necessitates special accommodations.
Description of Disability: [Describe the disability, its nature, severity, and any relevant medical information.]
Extent of Disability: [Explain the impact of the disability on daily life activities and any specific limitations.]
Duration of Disability: [Specify if the disability is temporary or permanent and provide the anticipated duration if applicable.]
This Disability Certificate is issued for the purpose of [Specify the purpose, e.g., availing government benefits, employment accommodations, etc.].
Date of Issuance: [Date] Expiry Date (if applicable): [Date] Doctor’s Signature: [Doctor’s Signature]
Format 3: Government-Issued Disability Certificate
[Official Government Logo/Heading] [Name of the Government Department/Agency] [Address of the Government Department] [City, State, ZIP Code] [Phone Number] [Website (if applicable)]
DISABILITY CERTIFICATE
[Government Seal/Stamp]
This is to certify that Mr./Ms. [Full Name of the Person] is recognized by [Name of the Government Department/Agency] as a person with a disability under the provisions of [Relevant Legislation or Regulation].
Description of Disability: [Describe the disability and provide any specific details required by the law.]
Extent of Disability: [Explain the impact of the disability on daily life activities and any specific limitations.]
Duration of Disability: [Specify if the disability is temporary or permanent and provide the anticipated duration if applicable.]
This Disability Certificate is issued for the purpose of [Specify the purpose, e.g., availing government benefits, employment accommodations, etc.].
Date of Issuance: [Date] Expiry Date (if applicable): [Date] Authorized Signature: [Authorized Signature]
Please note that the actual format and content of a Disability Certificate may vary depending on local regulations and the specific requirements of the issuing authority. It’s essential to consult with the relevant authority or medical professional for accurate and up-to-date information on Disability Certificate formats in your jurisdiction.
We write letters, applications, and email templates and create documents for our visitors at the semioffice. Please let us know in the comments if you need us to create a new letter, application, or email template. We will make it and publish it at semioffice and inform you accordingly.